
Clinical trials are the soul of any new human intervention. Many pharmaceutical and non-pharmaceutical products or interventions undergo clinical trials to test their human applicability. In this era of non-communicable diseases, most clinical trials run for an extended period of time. Survival analysis is an important analysis performed in most clinical trials that aim to capture time-to-event data. Various statistical data visualisation methods can perform time-to-event analysis.1 Kaplan-Meir analysis and Cox regression are the most commonly employed methods in survival analysis. Survival rates are the basic inference we try to get from any time-to-event analysis. The statistical tool is frequently used in numerous clinical trials, and nuances in interpreting this are essential for a researcher and a treating physician in this era of evidence-based medicine. The two common biases encountered in clinical trials that compare survival rates are as follows;
-
Lead-time bias
-
Length-time bias
This article aims to simplify the concept of lead-time and length-time bias, which is essential for adequately interpreting time-to-event analysis, especially for beginners.
Lead-time bias could be defined as "Any diagnostic or therapeutic modality that appears beneficial just because of the early diagnosis of the particular condition but doesn't possess any in reality."3 A simple example could very well explain the concept of lead-time bias. Let's assume we plan to conduct a clinical trial on cervical cancer. Our study intends to compare the efficacy of new chemotherapeutic agents with the existing standard of care. We have recruited 2000 participants and are trying to find the five-year survival rate between the two interest groups. Each group has 1,000 participants.
Another critical point is that I include all cervical cancer patients from stage I to IV to clarify this concept. The trial starts, and patients are randomised to their respective groups. In our treatment group, let's assume we have 700 patients diagnosed by screening for cervical cancer, and they belong to stages I and II.
On the other hand, in the standard-of-care group, we have 500 patients who belong to stages I and II, and the rest 500 participants belong to stages III and IV. In this scenario, the results turn out to be favourable for the treatment group. A beginner unaware of the lead-time bias concept will find the results exciting and feel that the new drug is doing wonders. In reality, the results are biased because of our participant selection. In the treatment group, 70 per cent had stage I and II disease. But in the standard-of-care group, only 50 per cent had stage I and II disease. Now let's assume all participants who had stage I and II diseases are alive, and all became censored observations in the Kaplan-Meir graph. And all the people with stages III and IV showed the event of interest, which is death in our case. If we compare both groups, the five-year survival will be 70 per cent with new drug therapy and 50 per cent with standard of care. The 20 per cent increment in the five-year survival rate is just because of the early diagnosis of the disease, that gave them extra time to live. The extra time gained is due to screening and not to the efficacy of our intervention. The spare time the patient gains here is called "Lead-time," When this creeps in to inflate the beneficial effects of treatment that are not valid in reality, we call it "Lead-time bias." To avoid this, we never compare any groups with varying disease severity. If you look into published clinical trial literature, they only compare groups with the same stage of the disease. If you must compare groups with different stages of the disease, you can stratify them according to disease severity and do the same.
Lead-time bias also plays a significant role in studies that compare biomarkers for screening. Let's understand with an example. Let's assume our team is working with a biomarker to diagnose Huntington's disease. Clinical diagnosis of Huntington’s disease usually occurs in the 3rd or 4th decade of life, and its severity and manifestation appear in the earlier part of life in subsequent generations. To date, there has been no effective treatment to prevent the progression of Huntington’s disease. We develop and test a biomarker in our study groups in such a scenario. The biomarker identifies the person prone to developing Huntington’s disease 30 years before so that we can prevent it from setting. Unfortunately, despite not having any treatment options to prevent the disease, the spare time we have attained through this biomarker-based diagnosis is useless, despite being fair enough. The lead time gained in this case adds to the person’s anxiety about developing the disease and deteriorates his mental health. Statistically, despite performing better, our biomarker success is due to lead-time bias and will not be a useful screening tool. The above scenario is another example of Lead-time bias encountered in diagnostics. So, interpreting such trial results should be done cautiously, considering that lead-time bias may creep in at any time.
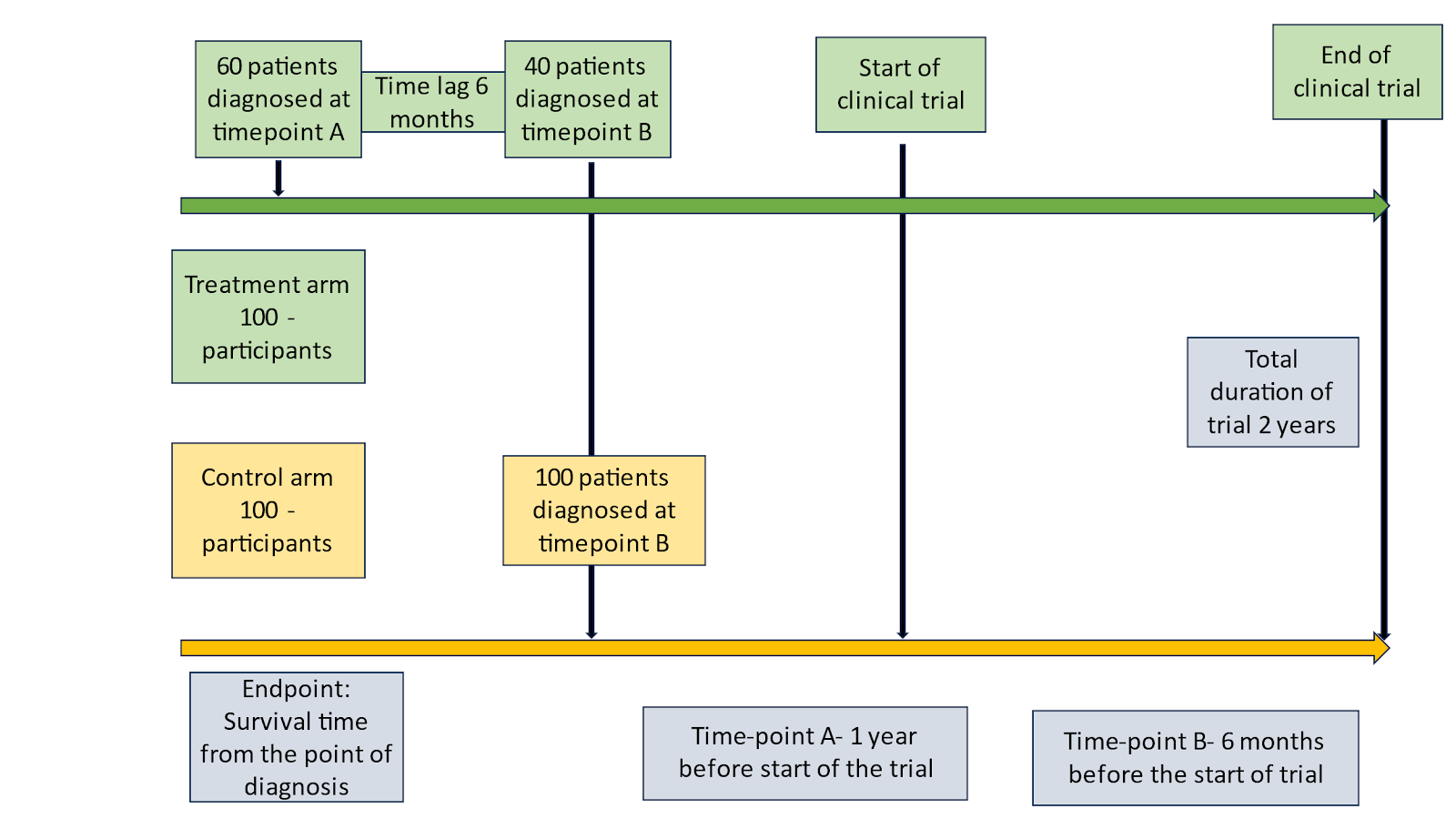
Figure 1: Lead-time bias in clinical trial
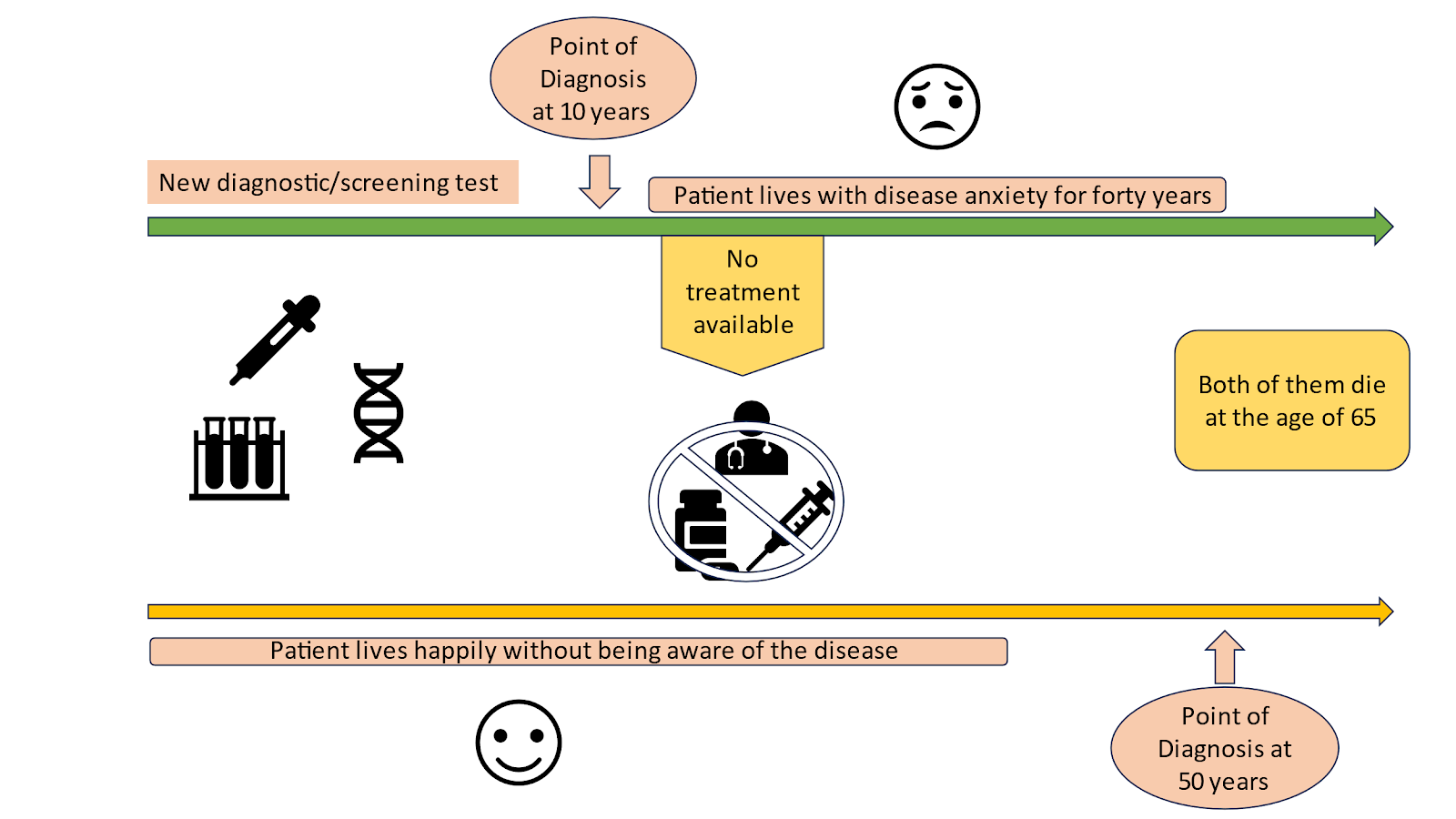
Figure 2: Lead-time bias in diagnostics
Length-time bias is another concept that must be considered when interpreting survival results. The concept of length-time bias is primarily concerned with comparing screening tests. Let’s understand this with an example. Our study team plans to develop a new screening tool for early detection of breast cancer. Breast cancer has numerous variants; some are low-grade malignancies that don’t affect the affected individuals' survival.




















Comments
0 comment