Klap: The AI Video Editing Tool Revolutionizing Social Media Content Creation
-

Field trips bring learning to life by connecting classroom lessons with rea...
Learn how to deploy voicebots in e-commerce to boost customer support, incr...
If you’ve ever heard the term ESR during a blood test, you might wonder wha...

حقن أوزمبيك هي علاج فعال يحتوي على مادة سيماغلوتايد، ويُستخدم أساسًا لتنظيم...

Discover the latest advancements in oncology services with our Breaking New...

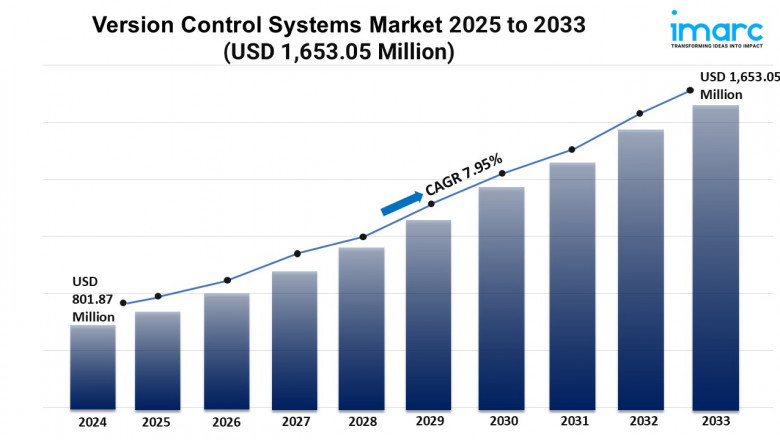
Government policies and infrastructure stimulus plans are key factors shapi...

According to Fortune Business Insights™, the global armored vehicle market...
Ontdek onze collectie kleine portemonnees voor dames. Perfect voor wie graa...